
Ohio Republicans Find Another Way to Erode Abortion Access (Updated)
Republican lawmakers in Ohio are going after telemedicine abortion and pushing a so-called abortion reversal bill as access to abortion care dwindles.
![[Photo: Flags fluttering outside of Ohio's Statehouse.]](https://rewirenewsgroup.com/wp-content/uploads/2020/01/ohio_1-800x533.jpg)
UPDATE, March 6, 2020, 3:56 p.m.: Ohio’s Republican-majority state senate on Wednesday passed Senate Bill 260, which would prohibit medication abortion via telemedicine, the Dayton Daily News reports.
Despite evidence that medication abortion is safe and effective, Ohio Republicans have introduced measures attacking the practice—further threatening access to abortion in a state where clinics are fighting to stay open.
State Sen. Steve Huffman (R-Tipp City) introduced a bill this week that would ban telemedicine abortions. This comes two months after the state senate approved legislation that would require physicians providing medication abortions to tell patients about “abortion reversal,” a medically dubious treatment promoted by anti-choice activists.
The bills are the latest salvo in the war Ohio anti-choice activists and politicians are waging against abortion.
Now some members of the Republican-dominated state legislature have turned their attention to making sure telemedicine abortion doesn’t take hold in the state. They’re following the lead of the 18 states that have telemedicine abortion bans and restrictions in place. In October, Republicans in the U.S. House of Representatives introduced federal legislation seeking to prohibit telemedicine abortion.
In a telemedicine abortion, the patient visits a health center that may not have a clinician on staff. The patient videoconferences with a clinician at another location who can answer questions and remotely authorize use of mifepristone and misoprostol, the two pills involved in a medication abortion. Medication abortions provided through telemedicine have been proven safe.
The clinics Rewire.News spoke to were not aware of any Ohio health center that publicly offers telemedicine abortion.
Ohio Right to Life, an anti-choice group that supports the proposed telemedicine abortion ban, cites the Food and Drug Administration’s Risk Evaluation and Mitigation Strategy (REMS) for mifepristone to cast medication abortion as dangerous. REMS is a regulatory tool the FDA uses to ensure extra care is taken when prescribing, dispensing, and taking drugs with an elevated risk. In mifepristone’s case, the REMS requires patients sign a consent form; that the prescribing clinician register with the drug manufacturer; and that the drug be dispensed at a doctor’s office, hospital, or clinic either by or under the supervision of the certified prescriber.
In fact, experts say the REMS is no longer necessary for mifepristone due to the drug’s proven track record since it was introduced in the United States in 2000. A 2017 study by researchers at Advancing New Standards in Reproductive Health (ANSIRH) analyzed 8,765 telemedicine and 10,405 in-person medication abortions, and found that adverse events were rare for both types of procedure; there was no statistically significant difference between them.
“We know from our epidemiological data that [mifepristone’s] safer than Tylenol,” Ushma Upadhyay, an associate professor at the University of California, San Francisco and a researcher for ANSIRH who has examined the impact of Ohio anti-choice laws, told Rewire.News. “It’s not based in evidence.”
Terri-Ann Thompson, a senior associate at Ibis Reproductive Health, agreed, adding that “removing [the REMS] would allow for other telehealth models be put into effect.”
While the telemedicine ban targets a safe procedure, the “abortion reversal” bill, which has not yet advanced in the Ohio House, would mandate telling patients about an unsafe one.
“Abortion reversal” is known to be harmful and lacks research into its efficacy, said Monica McLemore, a researcher with ANSIRH and associate professor at UCSF. McLemore called it “the bane of my existence.”
The first randomized control trial on so-called abortion reversal was canceled last year after several patients experienced hemorrhaging.
The Ohio clinics that Rewire.News spoke to said they were interested in using telemedicine to expand access to medication abortion. Other states’ experiences show that telemedicine can dramatically improve access. Maine’s growth in abortion clinics over the past decade was largely due to Maine Family Planning bringing telemedicine abortion to 17 of its clinics.
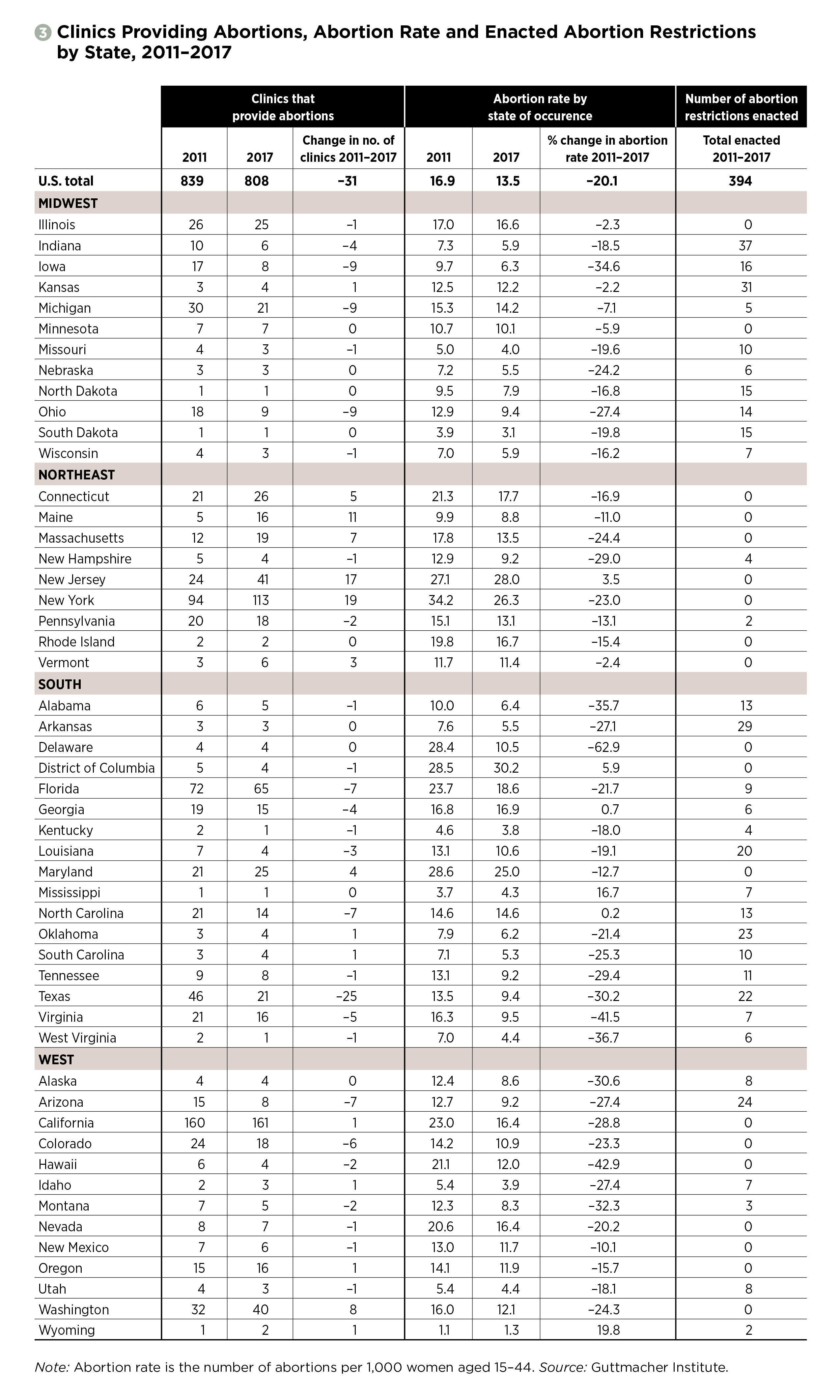
The proposed telemedicine ban would stymie any attempts by abortion providers in Ohio to do something similar in a state where a vast web of abortion restrictions have already diminished access and forced patients to travel to reach a provider. The anti-choice strategy of enacting medically unnecessary restrictions is working in Ohio: Nine abortion clinics closed between 2011 and 2017, according to the Guttmacher Institute. Upadhyay said there are large distances between the abortion clinics in Ohio, with the southwest corner of the state having the fewest clinics.
{kind=link}
The Republican-backed transfer agreement law, adopted in 2013, has been a particular burden to Ohio abortion providers. The law requires clinics to enter into an agreement with a local private hospital for transferring patients in case of complications. The law is unnecessary: If an abortion patient needed to seek emergency care at a hospital, the hospital would treat them even without an agreement.
Planned Parenthood’s Cincinnati Surgical Center, the only abortion clinic in the city, was recently threatened with closure after its variance—an official exemption to the transfer agreement, issued by the health department—was revoked. They have since been able to obtain a fourth back-up doctor necessary to keep their variance. Women’s Med Center of Dayton nearly closed last year for similar reasons.
Based on data from ANSIRH analyzed by Rewire.News, the loss of either clinic would significantly affect access for thousands in Ohio. Cincinnati Surgical Center is the closest abortion clinic for more than 500,000 women between ages 15 and 44. If the Cincinnati clinic were to close, those women would have to travel an extra 55 miles on average to reach the next closest clinic. For more than 300,000 women of reproductive age, Women’s Med Center of Dayton is the closest abortion clinic. If it were to close, they would be forced to travel an extra 66 miles on average to reach the next closest provider.
“Make no mistake, laws that restrict access like this written transfer agreement requirement are medically unnecessary and designed to prevent Ohioans from accessing basic reproductive health care,” Kersha Deibel, president and CEO of Planned Parenthood Southwest Ohio Region, said in a statement to Rewire.News. “Regardless, we jump through every hoop politicians put in our way in order to ensure patients can continue accessing safe, legal abortion in Ohio.”
Preterm, a Cleveland clinic, has largely avoided issues with obtaining a transfer agreement. But even in this ideal scenario, the requirement of a transfer agreement doesn’t help, said Chrisse France, Preterm’s executive director.
“As the state’s largest abortion provider, Preterm is lucky to have great relationships with many of the health-care institutions in the city,” France told Rewire.News. “However, the transfer agreement is an unnecessary provision designed specifically to shut down abortion clinics in Ohio. Shutting down abortion clinics in Ohio does not reduce the number of abortions, and transfer agreements don’t make what is already a very safe procedure safer. Instead, transfer agreements often shut down abortion clinics because of pressure on hospitals not to sign because of abortion stigma.”
Researchers agree.
“My sense is that the transfer agreement really only serves to perpetuate a myth that abortion is not safe,” Upadhyay told Rewire.News. She added that that law serves to “shutter clinics.”